
what you want and the other guy wants in negotiations is not the common good being dictated by some authoritarian figure who somehow knows what is good for you. It is personal action by two parties acting in their self-interest. Common Good is an elitist attempt at authoritarianism and should be opposed by free thinking Cal grads.GivemTheAxe said:Creeping Incrementalism said:
This is a great thread. It covers everything so well that I have to summarize it before making a few points of my own:
- The poster in Western Australia, looking in from the outside, effectively says nothing has really changed from when shut things down in March because athletes were transmitting this virus. Considering capital-S Science and capital-D Data, it is impractical to play football considering that -- TRUE!
- HOWEVER -- The shutdowns/lockdowns were never based on rational science in the first place and we won't have enough data until this is all over the cost-benefit analysis of shutting down a modern economy is a new thing and can't be effectively calculated ahead of time. _Fear_ has always been the over-riding factor behind the lockdown.
- The typical modern Western individual wasn't intellectually equipped to handle a for-real epidemic coming in to this, for example "Epidemic" was a term most commonly used with obesity. We haven't faced the threat of truly scary epidemic disease since the 50s with polio. So today, after a few months, people have finally learned a more reasonable risk-reward ratio and decided that they don't care if there is a 1 in a 100 chance of them dying, or a chance of a player dying that is 1-1000 or less... sure players/staff some will die, but did Agu's death stop football?
- If campus is open, the intellectual honesty to play football is also present.
As for this "common good" garbage -- we live in such a heterogeneous society in California that there is nothing in common anymore.
Totally disagree. Robert Reich wrote a piece about us regaining the Common Good. It is a concept that has been disparaged by people who benefit from dividing us. It is a concept that still exists and will remain as long as we try to focus on our similarities and not on our differences
Chancellor Tien took every effort to foster that feeling among Cal Students. That is why he was ever present at Cal FB and BB games. He said that was something all Cal students could get behind.
As a lawyer I often was involved in settlement negotiations. In order to accomplish my objectives, I looked for points of possible agreement and not disagreement. The point was to find something the side wanted and needed that I could provide in exchange for something I wanted and needed.
All UC campuses to open in the fall
21,799 Views |
107 Replies |
Last: 5 yr ago by BancroftBear93
Yep. Common interest bargaining in a union labor/management setting is the best way to resolve seemingly intractable issues. During my career, I was involved in labor negotiations in which we were able to get both sides to initially agree to focus on critical issues they considered topics of common interest. Building on the relationships developed during those discussions, both sides were able to successfully move forward to address the more thorny issues. Reich is correct. Focusing on the similarities is the key to moving processes towards a resolution that is mutually beneficial.GivemTheAxe said:Creeping Incrementalism said:
This is a great thread. It covers everything so well that I have to summarize it before making a few points of my own:
- The poster in Western Australia, looking in from the outside, effectively says nothing has really changed from when shut things down in March because athletes were transmitting this virus. Considering capital-S Science and capital-D Data, it is impractical to play football considering that -- TRUE!
- HOWEVER -- The shutdowns/lockdowns were never based on rational science in the first place and we won't have enough data until this is all over the cost-benefit analysis of shutting down a modern economy is a new thing and can't be effectively calculated ahead of time. _Fear_ has always been the over-riding factor behind the lockdown.
- The typical modern Western individual wasn't intellectually equipped to handle a for-real epidemic coming in to this, for example "Epidemic" was a term most commonly used with obesity. We haven't faced the threat of truly scary epidemic disease since the 50s with polio. So today, after a few months, people have finally learned a more reasonable risk-reward ratio and decided that they don't care if there is a 1 in a 100 chance of them dying, or a chance of a player dying that is 1-1000 or less... sure players/staff some will die, but did Agu's death stop football?
- If campus is open, the intellectual honesty to play football is also present.
As for this "common good" garbage -- we live in such a heterogeneous society in California that there is nothing in common anymore.
Totally disagree. Robert Reich wrote a piece about us regaining the Common Good. It is a concept that has been disparaged by people who benefit from dividing us. It is a concept that still exists and will remain as long as we try to focus on our similarities and not on our differences
Chancellor Tien took every effort to foster that feeling among Cal Students. That is why he was ever present at Cal FB and BB games. He said that was something all Cal students could get behind.
As a lawyer I often was involved in settlement negotiations. In order to accomplish my objectives, I looked for points of possible agreement and not disagreement. The point was to find something the side wanted and needed that I could provide in exchange for something I wanted and needed.
Oh Boy - I'm afraid this isn't going to endGrigsby said:
Oh boy.... this isn't going to end well.
edg64 said:Sorry I apologizeedg64 said:Oh boy.... I'm afraid this isn't going to endGrigsby said:
Oh boy.... this isn't going to end well.
I got 'zapped', but, I think I have destroyed the intrusion.
Bring back It’s It’s to Haas Pavillion!
wifeisafurd said:Rational science is constantly changing based on new information and observations. Changes in views also be affected by social, political or religious impacts. Did the Chinese or WHO slant data? What are government agendas? But IMO the reality seems to be Western medical experts didn't know all that much about COVID when it hit, did the best they could with limited and changing information, made some mistakes and changed their minds (lockdowns (remember initially our Federal experts were against them relying on the traditional herd immunity approach for flu), masks, risks from COVID on surfaces, etc.), and, at least in most cases, were led by what they could find out. That scientists changed their minds is a good thing.Creeping Incrementalism said:
This is a great thread. It covers everything so well that I have to summarize it before making a few points of my own:
- The poster in Western Australia, looking in from the outside, effectively says nothing has really changed from when shut things down in March because athletes were transmitting this virus. Considering capital-S Science and capital-D Data, it is impractical to play football considering that -- TRUE!
- HOWEVER -- The shutdowns/lockdowns were never based on rational science in the first place and we won't have enough data until this is all over the cost-benefit analysis of shutting down a modern economy is a new thing and can't be effectively calculated ahead of time. _Fear_ has always been the over-riding factor behind the lockdown.
- The typical modern Western individual wasn't intellectually equipped to handle a for-real epidemic coming in to this, for example "Epidemic" was a term most commonly used with obesity. We haven't faced the threat of truly scary epidemic disease since the 50s with polio. So today, after a few months, people have finally learned a more reasonable risk-reward ratio and decided that they don't care if there is a 1 in a 100 chance of them dying, or a chance of a player dying that is 1-1000 or less... sure players/staff some will die, but did Agu's death stop football?
- If campus is open, the intellectual honesty to play football is also present.
As for this "common good" garbage -- we live in such a heterogeneous society in California that there is nothing in common anymore.
As for a common good, it is hard to look at polls and see anything more than divisiveness currently. A shout out to Newsom who when dealing with COVID didn't really seem to go be drawn into politics the way some other politicians have. But in our society, markets and freedom of action make the common good, not some demigod.
71Bear said:Yep. Common interest bargaining in a union labor/management setting is the best way to resolve seemingly intractable issues. During my career, I was involved in labor negotiations in which we were able to get both sides to initially agree to focus on critical issues they considered topics of common interest. Building on the relationships developed during those discussions, both sides were able to successfully move forward to address the more thorny issues. Reich is correct. Focusing on the similarities is the key to moving processes towards a resolution that is mutually beneficial.GivemTheAxe said:Creeping Incrementalism said:
This is a great thread. It covers everything so well that I have to summarize it before making a few points of my own:
- The poster in Western Australia, looking in from the outside, effectively says nothing has really changed from when shut things down in March because athletes were transmitting this virus. Considering capital-S Science and capital-D Data, it is impractical to play football considering that -- TRUE!
- HOWEVER -- The shutdowns/lockdowns were never based on rational science in the first place and we won't have enough data until this is all over the cost-benefit analysis of shutting down a modern economy is a new thing and can't be effectively calculated ahead of time. _Fear_ has always been the over-riding factor behind the lockdown.
- The typical modern Western individual wasn't intellectually equipped to handle a for-real epidemic coming in to this, for example "Epidemic" was a term most commonly used with obesity. We haven't faced the threat of truly scary epidemic disease since the 50s with polio. So today, after a few months, people have finally learned a more reasonable risk-reward ratio and decided that they don't care if there is a 1 in a 100 chance of them dying, or a chance of a player dying that is 1-1000 or less... sure players/staff some will die, but did Agu's death stop football?
- If campus is open, the intellectual honesty to play football is also present.
As for this "common good" garbage -- we live in such a heterogeneous society in California that there is nothing in common anymore.
Totally disagree. Robert Reich wrote a piece about us regaining the Common Good. It is a concept that has been disparaged by people who benefit from dividing us. It is a concept that still exists and will remain as long as we try to focus on our similarities and not on our differences
Chancellor Tien took every effort to foster that feeling among Cal Students. That is why he was ever present at Cal FB and BB games. He said that was something all Cal students could get behind.
As a lawyer I often was involved in settlement negotiations. In order to accomplish my objectives, I looked for points of possible agreement and not disagreement. The point was to find something the side wanted and needed that I could provide in exchange for something I wanted and needed.
That is the basis of successful negotiation. Start by focusing on similarities and give some level of respect to the other side. If you begin by focusing on differences and no respect for the other side your negotiations are doomed to failure.
If you note that is how the constitution was negotiated. There were plenty of differences, animosity, suspicion Competition and and strife among the parties that came up with the Constitution.
It was NOT big group of friends singing kumbaya"
At many points it looked like failure was inevitable.
But they did come to a final resolution based upon the Common Good.
(Unfortunately their one big failure - dealing with Slavery - was the result of their mistaken belief that slavery would disappear as the tobacco economy disappeared and would not be allowed in the new states.)
Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Do we have to go over the history of the Constitution AGAIN? They didn't come to a final resolution based upon the Common Good, unless you say that the Common Good was embodied by the Constitution. You did fine until that point.GivemTheAxe said:71Bear said:Yep. Common interest bargaining in a union labor/management setting is the best way to resolve seemingly intractable issues. During my career, I was involved in labor negotiations in which we were able to get both sides to initially agree to focus on critical issues they considered topics of common interest. Building on the relationships developed during those discussions, both sides were able to successfully move forward to address the more thorny issues. Reich is correct. Focusing on the similarities is the key to moving processes towards a resolution that is mutually beneficial.GivemTheAxe said:Creeping Incrementalism said:
This is a great thread. It covers everything so well that I have to summarize it before making a few points of my own:
- The poster in Western Australia, looking in from the outside, effectively says nothing has really changed from when shut things down in March because athletes were transmitting this virus. Considering capital-S Science and capital-D Data, it is impractical to play football considering that -- TRUE!
- HOWEVER -- The shutdowns/lockdowns were never based on rational science in the first place and we won't have enough data until this is all over the cost-benefit analysis of shutting down a modern economy is a new thing and can't be effectively calculated ahead of time. _Fear_ has always been the over-riding factor behind the lockdown.
- The typical modern Western individual wasn't intellectually equipped to handle a for-real epidemic coming in to this, for example "Epidemic" was a term most commonly used with obesity. We haven't faced the threat of truly scary epidemic disease since the 50s with polio. So today, after a few months, people have finally learned a more reasonable risk-reward ratio and decided that they don't care if there is a 1 in a 100 chance of them dying, or a chance of a player dying that is 1-1000 or less... sure players/staff some will die, but did Agu's death stop football?
- If campus is open, the intellectual honesty to play football is also present.
As for this "common good" garbage -- we live in such a heterogeneous society in California that there is nothing in common anymore.
Totally disagree. Robert Reich wrote a piece about us regaining the Common Good. It is a concept that has been disparaged by people who benefit from dividing us. It is a concept that still exists and will remain as long as we try to focus on our similarities and not on our differences
Chancellor Tien took every effort to foster that feeling among Cal Students. That is why he was ever present at Cal FB and BB games. He said that was something all Cal students could get behind.
As a lawyer I often was involved in settlement negotiations. In order to accomplish my objectives, I looked for points of possible agreement and not disagreement. The point was to find something the side wanted and needed that I could provide in exchange for something I wanted and needed.
That is the basis of successful negotiation. Start by focusing on similarities and give some level of respect to the other side. If you begin by focusing on differences and no respect for the other side your negotiations are doomed to failure.
If you note that is how the constitution was negotiated. There were plenty of differences, animosity, suspicion Competition and and strife among the parties that came up with the Constitution.
It was NOT big group of friends singing kumbaya"
At many points it looked like failure was inevitable.
But they did come to a final resolution based upon the Common Good.
(Unfortunately their one big failure - dealing with Slavery - was the result of their mistaken belief that slavery would disappear as the tobacco economy disappeared and would not be allowed in the new states.)
The Founders' belief wasn't that slavery would disappear as the tobacco economy disappeared. It was that half the colonies would refuse to be part of the new nation if slavery was eliminated per force in the Constitution. They all knew that the northern colonies would then speak French and the southern ones would speak Spanish. They hammered out compromises that created the conditions under which the Civil War would succeed. The 3/5 rule was the first such. The second was the provision enabling the end of the slave trade (which came at the first opportunity in 1808, by the Congress and President Jefferson). When the remainder of slavery didn't dry up (repeated studies of the economics of slavery show that few planters broke even financially with slaves, let alone profited), the nation went all in to eliminate it 50 years later...one of the first nations to do so. The failure was in those planters (including Founders) who valued their slave assets over their stated moral principles that the practice was inhuman.
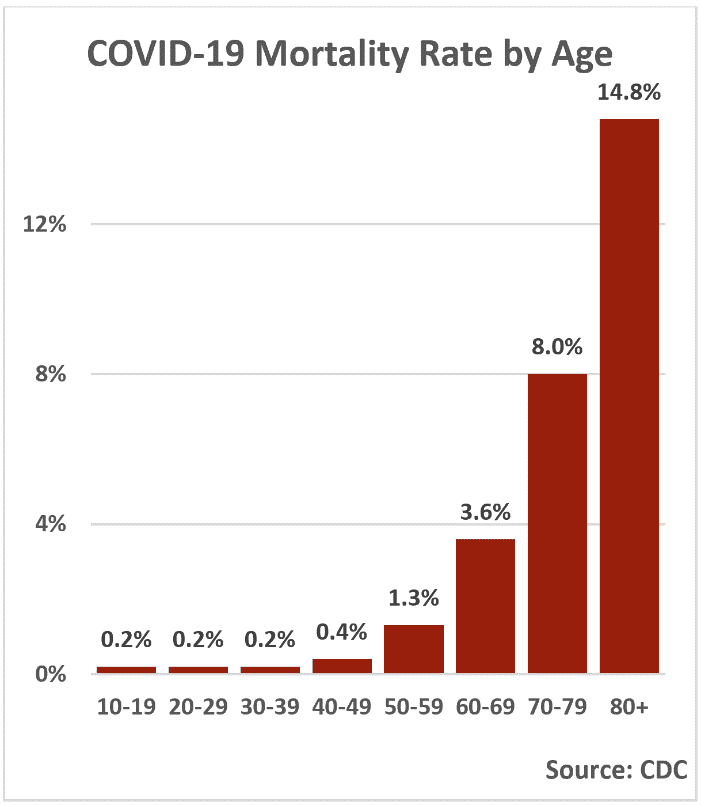
You know this post would be a lot better with cites to actual data. Like the CDC numbers (which btw, are actually reported cases as opposed to hypothetical cases, which I thought was discredited after that using the bull crap Stanford study model that 85% of everyone had COVID), unlike article in the next post about "actual" cases, as opposed to reported cases). I guess people just read articles with studies. Your risk of dying from Covid-19 rises with age. Here's how that compares with the flu or traffic crashes https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities via @bopinion Your understanding certainly doesn't comport with the tables.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
I'm with you on this one Unit. If Covid were even in the same ballpark as the seasonal flu, we wouldn't be in the soup in which we currently find ourselves. However, no matter what data is presented, there will always be a subsection of the population that denies it. It is the nature of the beast.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
The front page of this morning's New York Times is a sobering reminder that the pandemic is a killer to a degree not seen in our lifetimes. To toss it off as something akin to seasonal flu tells me more about the person that insists it is the case than anything else.
While COVID is more deadly, it is not more deadly to everyone. Saying no mater how the data is presented there must be deniers is a closed mind approach, which ignores huge differences in the death rates by demographics, particularly age. Ignorance is bliss.71Bear said:I'm with you on this one Unit. If Covid were even in the same ballpark as the seasonal flu, we wouldn't be in the soup in which we currently find ourselves. However, no matter what data is presented, there will always be a subsection of the population that denies it. It is the nature of the beast.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
The front page of this morning's New York Times is a sobering reminder that the pandemic is a killer to a degree not seen in our lifetimes. To toss it off as something akin to seasonal flu tells me more about the person that insists it is the case than anything else.
The reason why Fauci and Obama did not approve a quarantine for H1N1 was because the average age of people seriously impacted was far less than the average age of COVID. I guess they had it wrong looking at it by demographics.
I challenge you to look at a recent table of deaths by age and tell me that with 18 to 22 years olds, COVID is way above the death rate of seasonal flu. To flop off these demographic differences suggests someone who have become intellectually lazy about wanting to understand the true nature of the beast. I call you a denier for choosing to ignore these statistics.
For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. Looks like overall it is not 5-10 times deadlier more like 3 times and for the ages below 26 not much worse than flu/pneumonia perhaps 2:1. See Bloomberg article. https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalitiesCivil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
Granted, I did not provide a link to my source (because I couldn't recall where I read it), which is why I prefaced it with "if". But if you are going to accuse me and others of spreadings lies, the least you could do as a courtesy is cite your source.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
In case you missed the link posted by Goobear and Wifeisafurd:
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
Conversely, I challenge you to do the same.wifeisafurd said:While COVID is more deadly, it is not more deadly to everyone. Saying no mater how the data is presented there must be deniers is a closed mind approach, which ignores huge differences in the death rates by demographics, particularly age. Ignorance is bliss.71Bear said:I'm with you on this one Unit. If Covid were even in the same ballpark as the seasonal flu, we wouldn't be in the soup in which we currently find ourselves. However, no matter what data is presented, there will always be a subsection of the population that denies it. It is the nature of the beast.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
The front page of this morning's New York Times is a sobering reminder that the pandemic is a killer to a degree not seen in our lifetimes. To toss it off as something akin to seasonal flu tells me more about the person that insists it is the case than anything else.
The reason why Fauci and Obama did not approve a quarantine for H1N1 was because the average age of people seriously impacted was far less than the average age of COVID. I guess they had it wrong looking at it by demographics.
I challenge you to look at a recent table of deaths by age and tell me that with 18 to 22 years olds, COVID is way above the death rate of seasonal flu. To flop off these demographic differences suggests someone who have become intellectually lazy about wanting to understand the true nature of the beast. I call you a denier for choosing to ignore these statistics.
I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
Oak has quoted the actual numbers as of the date of his post. I have quoted CDC rates and posted an article with a table of CDC rates with COVID versus seasonal flu that simply shows your understanding is wrong. I realize '71 may not want to be bothered by statistics not related to total death rates for everyone, but the foundation to your argument is that there is a substantial higher death rates for COVID in 18 to 22 year olds, and further (though there are no numbers for this) 18 to 22 year olds in really good shape. The argument I would make is that you may want to assess individual players based on other criteria (sorry '71, yet another breakdown of stats) such as players with secondary risks, (e.g., do they have diabetes?), because (1) the numbers of deaths in young age groups is small, and (2) the numbers in deaths related to COVID and seasonal flu is fairly similar, and at different times of measurement the number related to season flu has been higher. But that is not your argument. BTW, the seasonal flu is not the "common flu" whatever that is in the spreading lies area. It is H1N1, and a myriad of other influenza viruses that are responsible for seasonal flu epidemics. I only point out H1N1 because it is particularly more deadly to those in the college age group that senior age groups, and still around killing people. When you say the evidence doesn't support that and you say people are spreading lies, you better come with some sources. I did. Oak did.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
Four things I take away from your chart:Unit2Sucks said:I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
1. The data is over 2 months old, which is everything in these changing times.
2. 20-44 is a very wide range, particularly to our discussion, and how the death rate for 19 yo's is zero.
3. Perhaps we should only allow underclassmen to play (I am being facetious).
4. Your data is not worthy of accusing me of spreading lies.
I suggest you use relevant data before calling people liars. 18 to 44 really? You couldn't find a larger grouping? . Why not look at the CDC chart in the article I posted which shows the death rates going through relevant age groups for both COVID and seasonal flu?Unit2Sucks said:I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
First - your original claim, to which I objected, was that the seasonal flu is deadlier than COVID to these kids. If someone can find me some data showing that COVID is less lethal than the seasonal flu for college age kids, I would be more than happy to apologize and correct myself. But I don't think you're going to be able to do that because, let's be honest, we all know it isn't true.Civil Bear said:Four things I take away from your chart:Unit2Sucks said:I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
1. The data is over 2 months old, which is everything in these changing times.
2. 20-44 is a very wide range, particularly to our discussion, and how the death rate for 19 yo's is zero.
3. Perhaps we should only allow underclassmen to play (I am being facetious).
4. Your data is not worthy of accusing me of spreading lies.
You haven't presented any data whatsoever showing the flu is deadlier than COVID for any age group. I've presented data that is 2 months old but the main purpose of sharing my data was to illustrate how unlikely a college kid is to die of the seasonal flu and I think that whether my data is 2 weeks old, 2 months old or 2 years old it will not change for the flu. As rare as it is for 20 year olds to die from COVID (and I acknowledge it's quite rare), it's much more rare to have someone that age die from the flu. I'm less confident in the COVID data from that timeframe, but nothing I've seen since then shows that 20 year olds are faring as well as the flu.
The CDC data I presented shows that we are looking at somewhere around 0.01 or 0.02% for the seasonal flu. That is 1 or 2 out of every 10k seasonal flu cases among people under 50. Like I said above, I haven't seen any data showing COVID as having that little mortality for that age group. I've seen 0.2% or 0.1% from a number of sources over time, but nothing remotely approaching one tenth of that which is where we are with seasonal flu. Here's another example:
For what it's worth, you can look at CDC data directly and do a bunch of different cuts. As of the most recent date, 51 males between 15-24 have died of COVID in the US since February and only 24 have died from the flu.
We also know that it's extremely rare for flu survivors to have any long term effects. We don't yet know that about COVID, but there is some cause for concern.
Funny thing is if you actually hit on CDC data in your link as of 5/26 you get 76 people between 15-26 and died from COVID and 46 died from influenza. That is a different of 30 over 1 million cases and 100,000 deaths. Which means using 2020 numbers, the death rate by age group actually was at of 5/24 was .00878. If you divide that equally by year, for 18 to 24, the entire risk is .00348. The 30 person delta works out to be .0003, which for most people sane people looks like approximately the same, like essentially a rounding error of next to no risk. Interestingly, speaking of things like error, the Bloomberg article which you keep ignoring compared the 2018 seasonal flu with COVID, where the numbers for seasonal influenza were higher. Why use 2018? The numbers for influenza deaths are underreported at this point due to typical time lag, while COVID numbers are being watched closely and reported more quickly. But let's talk about reporting bias:Unit2Sucks said:First - your original claim, to which I objected, was that the seasonal flu is deadlier than COVID to these kids. If someone can find me some data showing that COVID is less lethal than the seasonal flu for college age kids, I would be more than happy to apologize and correct myself. But I don't think you're going to be able to do that because, let's be honest, we all know it isn't true.Civil Bear said:Four things I take away from your chart:Unit2Sucks said:I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
1. The data is over 2 months old, which is everything in these changing times.
2. 20-44 is a very wide range, particularly to our discussion, and how the death rate for 19 yo's is zero.
3. Perhaps we should only allow underclassmen to play (I am being facetious).
4. Your data is not worthy of accusing me of spreading lies.
You haven't presented any data whatsoever showing the flu is deadlier than COVID for any age group. I've presented data that is 2 months old but the main purpose of sharing my data was to illustrate how unlikely a college kid is to die of the seasonal flu and I think that whether my data is 2 weeks old, 2 months old or 2 years old it will not change for the flu. As rare as it is for 20 year olds to die from COVID (and I acknowledge it's quite rare), it's much more rare to have someone that age die from the flu. I'm less confident in the COVID data from that timeframe, but nothing I've seen since then shows that 20 year olds are faring as well as the flu.
The CDC data I presented shows that we are looking at somewhere around 0.01 or 0.02% for the seasonal flu. That is 1 or 2 out of every 10k seasonal flu cases among people under 50. Like I said above, I haven't seen any data showing COVID as having that little mortality for that age group. I've seen 0.2% or 0.1% from a number of sources over time, but nothing remotely approaching one tenth of that which is where we are with seasonal flu. Here's another example:
For what it's worth, you can look at CDC data directly and do a bunch of different cuts. As of the most recent date, 51 males between 15-24 have died of COVID in the US since February and only 24 have died from the flu.
We also know that it's extremely rare for flu survivors to have any long term effects. We don't yet know that about COVID, but there is some cause for concern.
1) you used out of date data
2) you played games with the groupings ages
3) strangely, you decided to take males only, wonder why? Is 51 bigger than 25?
Why are more men dying from COVID-19? https://www.livescience.com/why-covid-19-more-severe-men.html
To demonstrate how perverse the so many more players will die argument has become, to quote the article, for those ages 1 through 24, even a wildly out-of-control Covid-19 pandemic that exceeded the worst-case scenarios and killed 5 million Americans would appear to pose less risk than cars and trucks and boats do in a normal year. Young people really truly do not seem to be in a lot of danger from Covid-19. It's not zero danger: A few kids are dying from the disease. But the risk they face from catching it at school appears to be much smaller than the risk they face from, say, getting to school. Which makes the arguments about risks of football players dying seem really hysterical.
Civil, i was referring to Units remark. Again, Bloomberg cites 3:1 for 25-34 year olds. It is 2:1 for 15-24 year olds. Unit uses the 0.1 % for flu, and you read the article re the NY study re Covid you can estimate .27% for Covid. Looks again 3:1 overall is becoming the max number.Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
Striking how statistics makes us all liars.
My concern lies beyond the players themselves and for the others who are not in a younger age group but contribute to making the football team go. For the player's loved ones who could be compromised. Should we argue they be forced to play be damned their extended personal situations? Where does one draw the line? Doing so at and around the individual seems glaringly ignorant of what a contagious disease really is, contagious.
Also, we are in the midst of the early stages of the pandemic for which we know very little about the disease and it's long term effects. If a person gets COVID and suffers lung damage only to contract influenza in three years and die, what really caused their death? No data is going to tell you what hasn't occurred yet. I would assume nobody here disagrees with the notion that we are still learning about this disease?
My concern lies beyond the players themselves and for the others who are not in a younger age group but contribute to making the football team go. For the player's loved ones who could be compromised. Should we argue they be forced to play be damned their extended personal situations? Where does one draw the line? Doing so at and around the individual seems glaringly ignorant of what a contagious disease really is, contagious.
Also, we are in the midst of the early stages of the pandemic for which we know very little about the disease and it's long term effects. If a person gets COVID and suffers lung damage only to contract influenza in three years and die, what really caused their death? No data is going to tell you what hasn't occurred yet. I would assume nobody here disagrees with the notion that we are still learning about this disease?
Before I lock this - a reminder that accusing people of "lying" is not okay here. You can politely say you don't believe something is correct, there is some confusion, etc.
I used the male data because we were talking about college football players. I thought that would be obvious. As for the other data you cite - it appears you aren't talking about the case fatality rate (which is the percentage of COVID patients who die) but rather the percentage of a population who die of either COVID or flu. These are two separate concepts.wifeisafurd said:Funny thing is if you actually hit on CDC data in your link as of 5/26 you get 76 people between 15-26 and died from COVID and 46 died from influenza. That is a different of 30 over 1 million cases. Which means using 2020 numbers, the death rate by age group actually was at of 5/24 was .000878. If you divide that equally by year, for 18 to 24, the entire risk is .000348. The 30 person delta works out to be .00003, which for most people sane people looks like approximately the same, like essentially a rounding error of next to no risk. Interestingly, speaking of things like error, the Bloomberg article which you keep ignoring compared the 2018 seasonal flu with COVID, where the numbers for seasonal influenza were higher. Why use 2018? The numbers for influenza deaths are underreported at this point due to typical time lag, while COVID numbers are being watched closely and reported more quickly. But let's talk about reporting bias:Unit2Sucks said:First - your original claim, to which I objected, was that the seasonal flu is deadlier than COVID to these kids. If someone can find me some data showing that COVID is less lethal than the seasonal flu for college age kids, I would be more than happy to apologize and correct myself. But I don't think you're going to be able to do that because, let's be honest, we all know it isn't true.Civil Bear said:Four things I take away from your chart:Unit2Sucks said:I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
1. The data is over 2 months old, which is everything in these changing times.
2. 20-44 is a very wide range, particularly to our discussion, and how the death rate for 19 yo's is zero.
3. Perhaps we should only allow underclassmen to play (I am being facetious).
4. Your data is not worthy of accusing me of spreading lies.
You haven't presented any data whatsoever showing the flu is deadlier than COVID for any age group. I've presented data that is 2 months old but the main purpose of sharing my data was to illustrate how unlikely a college kid is to die of the seasonal flu and I think that whether my data is 2 weeks old, 2 months old or 2 years old it will not change for the flu. As rare as it is for 20 year olds to die from COVID (and I acknowledge it's quite rare), it's much more rare to have someone that age die from the flu. I'm less confident in the COVID data from that timeframe, but nothing I've seen since then shows that 20 year olds are faring as well as the flu.
The CDC data I presented shows that we are looking at somewhere around 0.01 or 0.02% for the seasonal flu. That is 1 or 2 out of every 10k seasonal flu cases among people under 50. Like I said above, I haven't seen any data showing COVID as having that little mortality for that age group. I've seen 0.2% or 0.1% from a number of sources over time, but nothing remotely approaching one tenth of that which is where we are with seasonal flu. Here's another example:
For what it's worth, you can look at CDC data directly and do a bunch of different cuts. As of the most recent date, 51 males between 15-24 have died of COVID in the US since February and only 24 have died from the flu.
We also know that it's extremely rare for flu survivors to have any long term effects. We don't yet know that about COVID, but there is some cause for concern.
1) you used out of date data
2) you played games with the groupings ages
3) strangely, you decided to take males only, wonder why? Is 51 bigger than 25?
Why are more men dying from COVID-19? https://www.livescience.com/why-covid-19-more-severe-men.html
To demonstrate how perverse the so many more players will die argument has become, to quote the article, for those ages 1 through 24, even a wildly out-of-control Covid-19 pandemic that exceeded the worst-case scenarios and killed 5 million Americans would appear to pose less risk than cars and trucks and boats do in a normal year. Young people really truly do not seem to be in a lot of danger from Covid-19. It's not zero danger: A few kids are dying from the disease. But the risk they face from catching it at school appears to be much smaller than the risk they face from, say, getting to school. Which makes the arguments about risks of football players dying seem really hysterical.
As for my original point - there is no data which has shown the flu to be deadlier to college football player types (eg healthy males 18-24) than COVID. If we accept everyone's conclusions at face value, COVID is somewhere between just as lethal as the flu to 10x more lethal. I've tried my hardest to find any data to support the position that a college football player should be more concerned with contracting the seasonal flu than COVID and I just can't find anything, nor has anyone presented any data in that direction.
As for your new claim "To demonstrate how perverse the so many more players will die argument has become", that's not an argument that I've made (or that I can recall anyone else making in this thread). I specifically said that the mortality rate is "quite rare" and nowhere have I said otherwise. If I were a college football player, I wouldn't be worried about death, I would be worried about other potential impacts down the road from an adverse reaction. Heck, as it turns out I'm not a college football player and I have no concerns about myself dying from COVID - but I am worried about lung or other organ damage and I worry about this new MIS thing for my kids.
This is a reasonable comment. It is amazing how little was known when COVID hit and how are top scientists have changed their minds and developed protocols to reduce COVID spread. Now if only people will believe them and follow their recommendations. The reason flu's high fatality rate doesn't spur dread (so little, that fewer than half of U.S. adults get vaccinated) is its familiarity. The flu isn't novel, it happens every year, and it has some predictability" in terms of seasonality. Despite much better number currently in the US overall, we still don't know if COVID goes on a typical virus curve. Contributing to anxiety is confused and confusing pronouncements from elected officials, the media and even academic. COVID seemed to come out of nowhere (which may not be factually true thank you China and WHO), but the admitted unfamiliarity combines with the admitted uncertainty (we are still learning) to increase anxiety. In the face of an unfamiliar risk, erring on the side of extreme caution often is perceived as better, even if it has consequences.CALiforniALUM said:
Striking how statistics makes us all liars.
My concern lies beyond the players themselves and for the others who are not in a younger age group but contribute to making the football team go. For the player's loved ones who could be compromised. Should we argue they be forced to play be damned their extended personal situations? Where does one draw the line? Doing so at and around the individual seems glaringly ignorant of what a contagious disease really is, contagious.
Also, we are in the midst of the early stages of the pandemic for which we know very little about the disease and it's long term effects. If a person gets COVID and suffers lung damage only to contract influenza in three years and die, what really caused their death? No data is going to tell you what hasn't occurred yet. I would assume nobody here disagrees with the notion that we are still learning about this disease?
It is interesting that the long term impact cuts works both ways. In the comparison, you see at the CDC site they often add pneumonia and seasonal flu numberers together when comparing to COVID, which I did not do in my posts. But the flu often leads to pneumonia and lung damage from COVID may do likewise or lead to other long term issues. It seems clear that the risk from bad COVID outcomes is more slanted to those who are older, where we have had other viruses (e.g., H1N1) that went the other way and younger people were more susceptible. Yet we didn't impose the same restrictions on H1N1, we used, in this country, a herd immunity approach (other countries did impose quarantines).
There is the problem with dealing with the unknown risk. You can take precautions, but leaving your house subjects you to all sorts of risks you can't control. You don't know the risk of long term skin cancer due to global warming, the risk you may have a traffic accident that day, will you be a victim of a crime, etc.The brain also is not very good at separating risks to a population from personal risks. You can try to mitigate risks by being selective when you leave your house and your actions. We now have a pretty good idea who is more susceptible to COVID, and those individuals should take more precautions, such as being very careful about when and how they leave the house. Players are far less susceptible, but they also will face various protections like temperatures checks before practice, to reduce risks and isolate those with COVID. The alternative with COVID numbers going down is to have a new normal of never leaving your home because of uncertainty.
I understand the male population now. Duh.Unit2Sucks said:I used the male data because we were talking about college football players. I thought that would be obvious. As for the other data you cite - it appears you aren't talking about the case fatality rate (which is the percentage of COVID patients who die) but rather the percentage of a population who die of either COVID or flu. These are two separate concepts.wifeisafurd said:Funny thing is if you actually hit on CDC data in your link as of 5/26 you get 76 people between 15-26 and died from COVID and 46 died from influenza. That is a different of 30 over 1 million cases. Which means using 2020 numbers, the death rate by age group actually was at of 5/24 was .000878. If you divide that equally by year, for 18 to 24, the entire risk is .000348. The 30 person delta works out to be .00003, which for most people sane people looks like approximately the same, like essentially a rounding error of next to no risk. Interestingly, speaking of things like error, the Bloomberg article which you keep ignoring compared the 2018 seasonal flu with COVID, where the numbers for seasonal influenza were higher. Why use 2018? The numbers for influenza deaths are underreported at this point due to typical time lag, while COVID numbers are being watched closely and reported more quickly. But let's talk about reporting bias:Unit2Sucks said:First - your original claim, to which I objected, was that the seasonal flu is deadlier than COVID to these kids. If someone can find me some data showing that COVID is less lethal than the seasonal flu for college age kids, I would be more than happy to apologize and correct myself. But I don't think you're going to be able to do that because, let's be honest, we all know it isn't true.Civil Bear said:Four things I take away from your chart:Unit2Sucks said:I'm willing to accept that my data is wrong if there is evidence to the contrary, but this is what I was basing it on:Civil Bear said:I'm not sure why I would need to take the younger group into account, but regardless I never said anything about 5-10 times. Unit2Sucks cited those numbers, but in the wrong direction. I just said the risk of players dying from COVID is less likely. You purported to have facts to the contrary.Goobear said:It doesn't. Take the group before it into account as well. You will get to 2:1. That is a far cry from 5-10 times.....Civil Bear said:The Bloomberg article points to a 3:1 ratio of influenza/pneumonia deaths to Covid deaths for 15-24 year-olds. That was the number I recalled when I made my initial point.Goobear said:For ages under 65 the death rate is 0.09%. It could go to .27%. Now obviously the kids under 25 will be much lower. A Bloomerg article lays that out. Looks like dying from flu/pneumonia for those age groups vs Covid looks to be 1:1.5.Civil Bear said:Goobear said:Better yet, actual facts. See interesting info re NY City etc below.Unit2Sucks said:Civil Bear said:Healthy players risk serious injury every time they suit up, so in that regard JW puts all his players' health at risk every game and practice. The question is, what is the reasonable amount of risk? If the risk of players dying from COVID-19 is less than doing the same from the seasonal flu (which I understand to be true for the age group) then one would think the risk is reasonable.calwhoyou? said:
For example, if I were to have asked this board whether JW (or any recent Cal coach) would ever place his players' health at risk, each and every person on this board would say not. I recall vociferous defenses of the Cal coaching staff during the Ted Agu fallout. Everyone on this board agreed that that the coaches would not willfully do anything to put his life at risk. But some members on this board now argue that JW would absolutely willfully put his players' health at risk. Remember: JW would not only have to believe that each of his players would act responsibly over the course of the football season (e.g., essentially a self-quarantine to avoid infection), but that every single player on each other team would act responsibly (remember, Cal plays teams that play other teams that plays other teams...).
Where is this notion that COVID is less deadly than the flu for college kids? My understanding is the death rate for the flu for this age group is about 0.01% which would make COVID 5-10x deadlier and that's without taking into account the number of COVID recovered individuals who will have permanent damage to lungs and/or other organs, which is far more rare with the flu.
I'm not saying that COVID is a death sentence for college football players but can we please stop spreading the lie that it's no worse than (or in this case less deadly than!) the common flu. The evidence simply doesn't support that position.
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
Please point to the facts in your link comparing college age deaths. I couldn't find it.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities
I thought I was being clear, but I was referring to a person's chances of dying if they have contracted the flu vs having contracted COVID. The Bloomberg article doesn't seem to be talking about that, unless I missed it. The flu is far more common in a typical year than COVID has been - eg the CDC is estimating 39-56 million people had the flu this season.
1. The data is over 2 months old, which is everything in these changing times.
2. 20-44 is a very wide range, particularly to our discussion, and how the death rate for 19 yo's is zero.
3. Perhaps we should only allow underclassmen to play (I am being facetious).
4. Your data is not worthy of accusing me of spreading lies.
You haven't presented any data whatsoever showing the flu is deadlier than COVID for any age group. I've presented data that is 2 months old but the main purpose of sharing my data was to illustrate how unlikely a college kid is to die of the seasonal flu and I think that whether my data is 2 weeks old, 2 months old or 2 years old it will not change for the flu. As rare as it is for 20 year olds to die from COVID (and I acknowledge it's quite rare), it's much more rare to have someone that age die from the flu. I'm less confident in the COVID data from that timeframe, but nothing I've seen since then shows that 20 year olds are faring as well as the flu.
The CDC data I presented shows that we are looking at somewhere around 0.01 or 0.02% for the seasonal flu. That is 1 or 2 out of every 10k seasonal flu cases among people under 50. Like I said above, I haven't seen any data showing COVID as having that little mortality for that age group. I've seen 0.2% or 0.1% from a number of sources over time, but nothing remotely approaching one tenth of that which is where we are with seasonal flu. Here's another example:
For what it's worth, you can look at CDC data directly and do a bunch of different cuts. As of the most recent date, 51 males between 15-24 have died of COVID in the US since February and only 24 have died from the flu.
We also know that it's extremely rare for flu survivors to have any long term effects. We don't yet know that about COVID, but there is some cause for concern.
1) you used out of date data
2) you played games with the groupings ages
3) strangely, you decided to take males only, wonder why? Is 51 bigger than 25?
Why are more men dying from COVID-19? https://www.livescience.com/why-covid-19-more-severe-men.html
To demonstrate how perverse the so many more players will die argument has become, to quote the article, for those ages 1 through 24, even a wildly out-of-control Covid-19 pandemic that exceeded the worst-case scenarios and killed 5 million Americans would appear to pose less risk than cars and trucks and boats do in a normal year. Young people really truly do not seem to be in a lot of danger from Covid-19. It's not zero danger: A few kids are dying from the disease. But the risk they face from catching it at school appears to be much smaller than the risk they face from, say, getting to school. Which makes the arguments about risks of football players dying seem really hysterical.
As for my original point - there is no data which has shown the flu to be deadlier to college football player types (eg healthy males 18-24) than COVID. If we accept everyone's conclusions at face value, COVID is somewhere between just as lethal as the flu to 10x more lethal. I've tried my hardest to find any data to support the position that a college football player should be more concerned with contracting the seasonal flu than COVID and I just can't find anything, nor has anyone presented any data in that direction.
As for your new claim "To demonstrate how perverse the so many more players will die argument has become", that's not an argument that I've made (or that I can recall anyone else making in this thread). I specifically said that the mortality rate is "quite rare" and nowhere have I said otherwise. If I were a college football player, I wouldn't be worried about death, I would be worried about other potential impacts down the road from an adverse reaction. Heck, as it turns out I'm not a college football player and I have no concerns about myself dying from COVID - but I am worried about lung or other organ damage and I worry about this new MIS thing for my kids.
The pivot too long term impact is interesting. I don't think that anyone knows the long term impact on those healthy young people who might get COVID without experiencing major symptoms. It is like analogous to my children can't be outside on a team or sport because of the long term impact of air pollution. If your child has a predisposition to risk, such as asthma, you maybe feel different. But what you are essentially now arguing is fear of the unknown. There is no way to argue with that other than don't leave the house - see my post above.
from left field punching up obvious incomparables..
o timely flu vaccinations are cheap safe and (mostly) effective.
o for covid none yet exists / may never be found.
# oski save us from lawyer-ing
o timely flu vaccinations are cheap safe and (mostly) effective.
o for covid none yet exists / may never be found.
# oski save us from lawyer-ing
muting more than 300 handles, turnaround is fair play
yeah but did they consult with the SIP fundamentalists on BI first?
yes, but in the hysteria of football players dying or having long term impacts, did you forget to consider the majority of adults don't even get flu vaccinations? Did you consider there are not vaccines for many flu strains? You better not leave your house, you may be infected.smh said:
from left field punching up obvious incomparables..
o timely flu vaccinations are cheap safe and (mostly) effective.
o for covid none yet exists / may never be found.
# oski save us from lawyer-ing
#oskisaveusfromhystericalpeople
Covid 19 does not seem to mutate to the extent the flu does. While a vaccine will not guarantee 100% safety,it would at least instill some confidence that the odds of getting it would be much less. I would take that risk which I am not willing to take now.
Bring back It’s It’s to Haas Pavillion!
Featured Stories
See All
Cal Football Spring Game Set For April 18
by Cal Athletics
4 Star Sierra Canyon Safety Myles Baker Commits to Cal
by Jim McGill
The Benson Blog - Postseason Awards
by Rod Benson
Cal Football Recruiting Focus: 2027 Wide Receivers
by Jim McGill