
The CDC Foundation funds online propaganda efforts to mass report and de-license doctors who they deem to be conveying 'misinformation', which it defines as anything contrary to CDC or WHO dogma. https://t.co/jVYvfP9oPw
— Jay Bhattacharya (@DrJBhattacharya) April 12, 2023
Vaccine Redux - Vax up and go to Class
1,162,150 Views |
6329 Replies |
Last: 11 days ago by sycasey
Probably because major medical journals have tougher peer review before publishing.movielover said:Healthy, athletic 14 yo girl dies 2 days post Pfizer dose 3 diagnosed w/"vaccine-related multiple-organ inflammation."
— Tracy Høeg, MD, PhD (@TracyBethHoeg) April 10, 2023
Why are healthy children being told to get a booster & why is this published in "Legal Medicine" instead of a major medical journal?https://t.co/XRZccJvkSJ pic.twitter.com/S0YjDbyAnC
This *may* explain a lot.
https://twitter.com/i/web/status/1647082019501879298
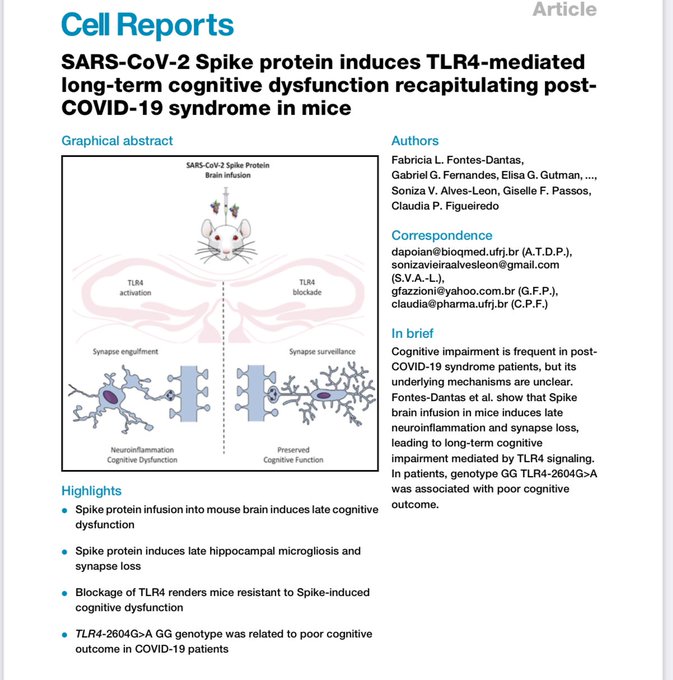
New paper demonstrates that exposure to Spike protein causes the destruction of synapses in the brain, neuro-inflammation, memory loss, and cognitive dysfunction 30-45 days after exposure. This neurotoxicity of the Spike protein appears to be mediated by TLR4, and is therefore a byproduct of the immune response to Spike.
[url=https://twitter.com/ScienceWDrDoug/status/1647082019501879298/photo/1][/url]
[url=https://twitter.com/ScienceWDrDoug/status/1647082019501879298/photo/1][/url]
https://twitter.com/i/web/status/1647082019501879298
New paper demonstrates that exposure to Spike protein causes the destruction of synapses in the brain, neuro-inflammation, memory loss, and cognitive dysfunction 30-45 days after exposure. This neurotoxicity of the Spike protein appears to be mediated by TLR4, and is therefore a byproduct of the immune response to Spike.
[url=https://twitter.com/ScienceWDrDoug/status/1647082019501879298/photo/1][/url]
[url=https://twitter.com/ScienceWDrDoug/status/1647082019501879298/photo/1][/url]
Damar Hamlin fulling cleared to resume football.
https://www.espn.com/nfl/story/_/id/36224496/bills-damar-hamlin-ok-play-suffering-cardiac-arrest
https://www.espn.com/nfl/story/_/id/36224496/bills-damar-hamlin-ok-play-suffering-cardiac-arrest
haha Director of National Intelligence, and Secretary of State was telling people this COVID thing came from a lab. Fauci was out calling them conspiracy theorists and Fauci never once talked with the DNI or SoS the whole time. The only thing you can take from that is Fauci was trying to cover up that he was funding that lab.
Also
Exactly
— Elon Musk (@elonmusk) April 18, 2023
Also
The monovalent Moderna and Pfizer-BioNTech COVID-19 vaccines are no longer authorized for use in the United States.
— U.S. FDA (@US_FDA) April 18, 2023
stuff MSB accidently left out..
https://www.nytimes.com/2023/04/18/health/covid-booster-shots-seniors.html
/****
The Food and Drug Administration on Tuesday authorized an additional round of bivalent booster shots for adults who are 65 and over as well as people with compromised immune systems. The effort is to ensure ongoing protection against Covid, which is still claiming more than 1,300 lives each week.
The bivalent shots target Omicron variants of the coronavirus. The agency said people who are 65 and older who have not had a bivalent booster shot in at least four months may get another one. For those who are immunocompromised, additional doses of the bivalent vaccine can be given two months after the last shot. Those who are unvaccinated can get a single dose of the bivalent booster, the agency said.
***/
https://www.nytimes.com/2023/04/18/health/covid-booster-shots-seniors.html
/****
The Food and Drug Administration on Tuesday authorized an additional round of bivalent booster shots for adults who are 65 and over as well as people with compromised immune systems. The effort is to ensure ongoing protection against Covid, which is still claiming more than 1,300 lives each week.
The bivalent shots target Omicron variants of the coronavirus. The agency said people who are 65 and older who have not had a bivalent booster shot in at least four months may get another one. For those who are immunocompromised, additional doses of the bivalent vaccine can be given two months after the last shot. Those who are unvaccinated can get a single dose of the bivalent booster, the agency said.
***/
Why?
— Elon Musk (@elonmusk) April 18, 2023
Hi, Elon. Thanks for your question. It's probably worth clarifying that the monovalent vaccines are still approved (licensed). That hasn't changed. But they are no longer authorized for *emergency use* in the United States.
— U.S. FDA (@US_FDA) April 18, 2023
?
There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Then fire her.
MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Medical or surgical masksdimitrig said:MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Published Jan 30 2023
https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses
Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people). Unwanted effects were rarely reported; discomfort was mentioned.
N95/P2 respirators
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people). Unwanted effects were not well-reported; discomfort was mentioned.
MinotStateBeav said:Medical or surgical masksdimitrig said:MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Published Jan 30 2023
https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses
Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people). Unwanted effects were rarely reported; discomfort was mentioned.
N95/P2 respirators
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people). Unwanted effects were not well-reported; discomfort was mentioned.
I'm sure it was just an oversight that you didn't post this bit, which comes immediately after the parts that you did post:
"What are the limitations of the evidence?
Our confidence in these results is generally low to moderate for the subjective outcomes related to respiratory illness, but moderate for the more precisely defined laboratory-confirmed respiratory virus infection, related to masks and N95/P2 respirators."
Why must you be so disingenuous? Is it intentional or are you blinded to your selectivity? I don't understand why you want to have discussions in such bad faith. It's a bad look that you shouldn't be proud of and should work to address if you are truly interested in having any kind of meaningful discussion.
I literally posted the link..so not really. Having moderate confidence is pretty good considering all the studies.Haloski said:MinotStateBeav said:Medical or surgical masksdimitrig said:MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Published Jan 30 2023
https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses
Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people). Unwanted effects were rarely reported; discomfort was mentioned.
N95/P2 respirators
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people). Unwanted effects were not well-reported; discomfort was mentioned.
I'm sure it was just an oversight that you didn't post this bit, which comes immediately after the parts that you did post:
"What are the limitations of the evidence?
Our confidence in these results is generally low to moderate for the subjective outcomes related to respiratory illness, but moderate for the more precisely defined laboratory-confirmed respiratory virus infection, related to masks and N95/P2 respirators."
Why must you be so disingenuous? Is it intentional or are you blinded to your selectivity? I don't understand why you want to have discussions in such bad faith. It's a bad look that you shouldn't be proud of and should work to address if you are truly interested in having any kind of meaningful discussion.
MinotStateBeav said:I literally posted the link..so not really. Having moderate confidence is pretty good considering all the studies.Haloski said:MinotStateBeav said:Medical or surgical masksdimitrig said:MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Published Jan 30 2023
https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses
Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people). Unwanted effects were rarely reported; discomfort was mentioned.
N95/P2 respirators
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people). Unwanted effects were not well-reported; discomfort was mentioned.
I'm sure it was just an oversight that you didn't post this bit, which comes immediately after the parts that you did post:
"What are the limitations of the evidence?
Our confidence in these results is generally low to moderate for the subjective outcomes related to respiratory illness, but moderate for the more precisely defined laboratory-confirmed respiratory virus infection, related to masks and N95/P2 respirators."
Why must you be so disingenuous? Is it intentional or are you blinded to your selectivity? I don't understand why you want to have discussions in such bad faith. It's a bad look that you shouldn't be proud of and should work to address if you are truly interested in having any kind of meaningful discussion.
Of course you posted the link. What else were you going to do? Quote and say where it was from without posting a link? Same difference, if you will. Anything else and you're not attributing it to anything, which just makes it a bunch of words without backing at all.
You just didn't bother to include that very important part of the piece I posted while using some excerpts as evidence for your apparent "side" here. That's not great, guy.
…and while you may post here that "having moderate confidence is pretty good considering all the studies," the actual people that performed the review don't feel the same way you do:
https://www.cochrane.org/news/statement-physical-interventions-interrupt-or-reduce-spread-respiratory-viruses-review
Of course, that was obvious based on the wording of the review itself.
TLDR: stop being disingenuous. You look silly.
I stand by what I posted, so TLDR: take a long walk off a short pier.Haloski said:MinotStateBeav said:I literally posted the link..so not really. Having moderate confidence is pretty good considering all the studies.Haloski said:MinotStateBeav said:Medical or surgical masksdimitrig said:MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Published Jan 30 2023
https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses
Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people). Unwanted effects were rarely reported; discomfort was mentioned.
N95/P2 respirators
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people). Unwanted effects were not well-reported; discomfort was mentioned.
I'm sure it was just an oversight that you didn't post this bit, which comes immediately after the parts that you did post:
"What are the limitations of the evidence?
Our confidence in these results is generally low to moderate for the subjective outcomes related to respiratory illness, but moderate for the more precisely defined laboratory-confirmed respiratory virus infection, related to masks and N95/P2 respirators."
Why must you be so disingenuous? Is it intentional or are you blinded to your selectivity? I don't understand why you want to have discussions in such bad faith. It's a bad look that you shouldn't be proud of and should work to address if you are truly interested in having any kind of meaningful discussion.
Of course you posted the link. What else were you going to do? Quote and say where it was from without posting a link? Same difference, if you will. Anything else and you're not attributing it to anything, which just makes it a bunch of words without backing at all.
You just didn't bother to include that very important part of the piece I posted while using some excerpts as evidence for your apparent "side" here. That's not great, guy.
…and while you may post here that "having moderate confidence is pretty good considering all the studies," the actual people that performed the review don't feel the same way you do:
https://www.cochrane.org/news/statement-physical-interventions-interrupt-or-reduce-spread-respiratory-viruses-review
Of course, that was obvious based on the wording of the review itself.
TLDR: stop being disingenuous. You look silly.
Here's the thing: that is just one study. Part of the reason these researchers can have only "moderate" confidence in the results is that individual studies with particular samples can produce weird results. You need to evaluate a full suite of them to really feel confident in drawing conclusions. Propagandists will hold up a weird outlier study and claim that it's the real truth.MinotStateBeav said:I stand by what I posted, so TLDR: take a long walk off a short pier.Haloski said:MinotStateBeav said:I literally posted the link..so not really. Having moderate confidence is pretty good considering all the studies.Haloski said:MinotStateBeav said:Medical or surgical masksdimitrig said:MinotStateBeav said:Maybe because as a society demonized people who spoke truth, you silenced them, you yelled at them in stores. We made up the fact that masks helped, that 6 feet distance would help (totally made up by the gov't btw) and that the vax would stop the spread. Social media blocked anything that went against orthodoxy, and kicked people off their platforms. You're killing grandma!!! So yeah..maybe we should look back at that massive f up. Because it was all led by your government. (including Trump's admin btw), with the media being uncritical government mouthpieces.Eastern Oregon Bear said:I wish you and others would put as much energy into figuring out where we should go from here as you do in looking backwards to assign blame and seek retribution.MinotStateBeav said:There was no "evolution of the science". Many scientists worldwide knew that the vax does not stop transmission by spring/summer 2021. The 2020 clinical trials did not check for transmission-blocking. https://t.co/319X98oDBZ
— Jay Bhattacharya (@DrJBhattacharya) April 19, 2023
If this is true, Walensky was lying to the public the whole time! So shocking.
Masks do help. People would pay more attention to RWNJs if they spent more time researching facts and less time spouting lies.
Published Jan 30 2023
https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses
Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people). Unwanted effects were rarely reported; discomfort was mentioned.
N95/P2 respirators
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people). Unwanted effects were not well-reported; discomfort was mentioned.
I'm sure it was just an oversight that you didn't post this bit, which comes immediately after the parts that you did post:
"What are the limitations of the evidence?
Our confidence in these results is generally low to moderate for the subjective outcomes related to respiratory illness, but moderate for the more precisely defined laboratory-confirmed respiratory virus infection, related to masks and N95/P2 respirators."
Why must you be so disingenuous? Is it intentional or are you blinded to your selectivity? I don't understand why you want to have discussions in such bad faith. It's a bad look that you shouldn't be proud of and should work to address if you are truly interested in having any kind of meaningful discussion.
Of course you posted the link. What else were you going to do? Quote and say where it was from without posting a link? Same difference, if you will. Anything else and you're not attributing it to anything, which just makes it a bunch of words without backing at all.
You just didn't bother to include that very important part of the piece I posted while using some excerpts as evidence for your apparent "side" here. That's not great, guy.
…and while you may post here that "having moderate confidence is pretty good considering all the studies," the actual people that performed the review don't feel the same way you do:
https://www.cochrane.org/news/statement-physical-interventions-interrupt-or-reduce-spread-respiratory-viruses-review
Of course, that was obvious based on the wording of the review itself.
TLDR: stop being disingenuous. You look silly.
AFAIK, the full suite of studies shows that yes, wearing a mask does reduce your chance to either catch or spread a respiratory virus. This seems pretty intuitively obvious: wearing something in front of your nose and mouth all the time is probably going to block at least some of the virus from going in or out. Where people might get confused is that there is also decent evidence that mask mandates didn't have a lot of effect in the US, in part because people didn't really follow them. The debate over mandates is more a public-policy question than a scientific one, though. The science shows that mask wearing does reduce spread, if people actually do it.
If you want to nitpick the wording of some of the conclusions, knock your socks off, but I think you're missing the big picture. We've been told over and over that the gold standard is RCTs. The vaccines are "safe and effective", the RCTs said so. The Ivermectin evidence is inconclusive; the clinical experience of real doctors saving actual patients is nothing compared to our (rigged) RCT. So if RCTs are the standard, it seems reasonable that we should accept the results of mask RCTs and let the evidence dictate what we believe is true and what policy should be rather than the other way around.
With this Cochrane study, we now we have a comprehensive review of dozens of studies including RCTs, and the data itself says that we cannot say that masks prevent transmission. That's how these things work. It's not question of maybe; the results are in and the answer is NO. If you refuse to accept that, then you might as well throw out every RCT including those of the beloved Covid vaxxines. "Science" remember. So let's compare that to the official narrative which is that masks are effective for respiratory viruses like Covid. That narrative is false and in fact was known to be false long before Covid. Remember those bogus non-controlled studies trumpeted by the CDC during the pandemic? That was misinformation. Studies for years have shown this (some of them are in the Cochrane review IIRC) and Fauci famously said as much on CBS and in private correspondence at the beginning of the pandemic.
You still think the Cochrane study still suggests masks are effective? Let's dig deeper.
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people).
Think about what this is saying. Do we really think the cloth masks grandma and little Joey were wearing in various improper ways made any difference whatsoever?
Check out this presentation by an industrial hygienist on the failure of masks, especially slides 21-22, and ask that question again.
https://granitegrok.com/wp-content/uploads/2022/04/1_Petty_New_Hampshire_Legislature_Presentation_January_27_2022.pdf
They lied to us. They lied to us to stoke fear and create a compliant, obedient populus, and it worked. When I pick up my kid at the high school, I still see healthy teenagers wearing masks...outside on a sunny day. WTH.
The fearmongering for control purposes was reason enough to decry the mask mandates, but that's just the tip of the iceberg. They completely ignored the negative side effects of the masks. Children especially need to see facial expressions. My sister, a speech pathologist, tells me there is an explosion of kids with speech problems due in large part to the masks. Then there is the medical consequences of masking, again completely ignored by the authoritarian medical narrative spinners. Granted, these effects are not experienced by everyone, but the masks mandates were inescapable regardless of a person's health condition and ability to cope with them. (see research below)
I'm not one of those raging anti-maskers. I complied without a fuss just like most people because even though I knew it was not protecting me or anyone else, the masks were a minor inconvenience and it made other people feel safer. But that in no way excuses what the authoritarian health czars did. The masks were not effective, they caused harm, and they divided the country. It was a stupid, cynical policy that set back trust (and rightly so) in our health authorities. And people wonder why wild conspiracy theories flourish. This is a major reason. Average folks can't evaluate the evidence for themselves, but they do know that they have been lied to and cannot trust the system so they are susceptible to any crazy idea that they find on the internet. And be assured, when there is a real medical threat, and the authorities actually are telling the truth, these people won't be listening then either. Once credibility is lost, it's very hard to regain. The boy cried wolf one too many times.
https://www.frontiersin.org/articles/10.3389/fpubh.2023.1125150/full
Background: As face masks became mandatory in most countries during the COVID-19 pandemic, adverse effects require substantiated investigation.
Methods: A systematic review of 2,168 studies on adverse medical mask effects yielded 54 publications for synthesis and 37 studies for meta-analysis (on n = 8,641, m = 2,482, f = 6,159, age = 34.8 12.5). The median trial duration was only 18 min (IQR = 50) for our comprehensive evaluation of mask induced physio-metabolic and clinical outcomes.
Results: We found significant effects in both medical surgical and N95 masks, with a greater impact of the second. These effects included decreased SpO2 (overall Standard Mean Difference, SMD = 0.24, 95% CI = 0.38 to 0.11, p < 0.001) and minute ventilation (SMD = 0.72, 95% CI = 0.99 to 0.46, p < 0.001), simultaneous increased in blood-CO2 (SMD = +0.64, 95% CI = 0.310.96, p < 0.001), heart rate (N95: SMD = +0.22, 95% CI = 0.030.41, p = 0.02), systolic blood pressure (surgical: SMD = +0.21, 95% CI = 0.030.39, p = 0.02), skin temperature (overall SMD = +0.80 95% CI = 0.231.38, p = 0.006) and humidity (SMD +2.24, 95% CI = 1.323.17, p < 0.001). Effects on exertion (overall SMD = +0.9, surgical = +0.63, N95 = +1.19), discomfort (SMD = +1.16), dyspnoea (SMD = +1.46), heat (SMD = +0.70), and humidity (SMD = +0.9) were significant in n = 373 with a robust relationship to mask wearing (p < 0.006 to p < 0.001). Pooled symptom prevalence (n = 8,128) was significant for: headache (62%, p < 0.001), acne (38%, p < 0.001), skin irritation (36%, p < 0.001), dyspnoea (33%, p < 0.001), heat (26%, p < 0.001), itching (26%, p < 0.001), voice disorder (23%, p < 0.03), and dizziness (5%, p = 0.01).
Discussion: Masks interfered with O2-uptake and CO2-release and compromised respiratory compensation. Though evaluated wearing durations are shorter than daily/prolonged use, outcomes independently validate mask-induced exhaustion-syndrome (MIES) and down-stream physio-metabolic disfunctions. MIES can have long-term clinical consequences, especially for vulnerable groups. So far, several mask related symptoms may have been misinterpreted as long COVID-19 symptoms. In any case, the possible MIES contrasts with the WHO definition of health.
Conclusion: Face mask side-effects must be assessed (risk-benefit) against the available evidence of their effectiveness against viral transmissions. In the absence of strong empirical evidence of effectiveness, mask wearing should not be mandated let alone enforced by law.
With this Cochrane study, we now we have a comprehensive review of dozens of studies including RCTs, and the data itself says that we cannot say that masks prevent transmission. That's how these things work. It's not question of maybe; the results are in and the answer is NO. If you refuse to accept that, then you might as well throw out every RCT including those of the beloved Covid vaxxines. "Science" remember. So let's compare that to the official narrative which is that masks are effective for respiratory viruses like Covid. That narrative is false and in fact was known to be false long before Covid. Remember those bogus non-controlled studies trumpeted by the CDC during the pandemic? That was misinformation. Studies for years have shown this (some of them are in the Cochrane review IIRC) and Fauci famously said as much on CBS and in private correspondence at the beginning of the pandemic.
You still think the Cochrane study still suggests masks are effective? Let's dig deeper.
Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people).
Think about what this is saying. Do we really think the cloth masks grandma and little Joey were wearing in various improper ways made any difference whatsoever?
Check out this presentation by an industrial hygienist on the failure of masks, especially slides 21-22, and ask that question again.
https://granitegrok.com/wp-content/uploads/2022/04/1_Petty_New_Hampshire_Legislature_Presentation_January_27_2022.pdf
They lied to us. They lied to us to stoke fear and create a compliant, obedient populus, and it worked. When I pick up my kid at the high school, I still see healthy teenagers wearing masks...outside on a sunny day. WTH.
The fearmongering for control purposes was reason enough to decry the mask mandates, but that's just the tip of the iceberg. They completely ignored the negative side effects of the masks. Children especially need to see facial expressions. My sister, a speech pathologist, tells me there is an explosion of kids with speech problems due in large part to the masks. Then there is the medical consequences of masking, again completely ignored by the authoritarian medical narrative spinners. Granted, these effects are not experienced by everyone, but the masks mandates were inescapable regardless of a person's health condition and ability to cope with them. (see research below)
I'm not one of those raging anti-maskers. I complied without a fuss just like most people because even though I knew it was not protecting me or anyone else, the masks were a minor inconvenience and it made other people feel safer. But that in no way excuses what the authoritarian health czars did. The masks were not effective, they caused harm, and they divided the country. It was a stupid, cynical policy that set back trust (and rightly so) in our health authorities. And people wonder why wild conspiracy theories flourish. This is a major reason. Average folks can't evaluate the evidence for themselves, but they do know that they have been lied to and cannot trust the system so they are susceptible to any crazy idea that they find on the internet. And be assured, when there is a real medical threat, and the authorities actually are telling the truth, these people won't be listening then either. Once credibility is lost, it's very hard to regain. The boy cried wolf one too many times.
https://www.frontiersin.org/articles/10.3389/fpubh.2023.1125150/full
Background: As face masks became mandatory in most countries during the COVID-19 pandemic, adverse effects require substantiated investigation.
Methods: A systematic review of 2,168 studies on adverse medical mask effects yielded 54 publications for synthesis and 37 studies for meta-analysis (on n = 8,641, m = 2,482, f = 6,159, age = 34.8 12.5). The median trial duration was only 18 min (IQR = 50) for our comprehensive evaluation of mask induced physio-metabolic and clinical outcomes.
Results: We found significant effects in both medical surgical and N95 masks, with a greater impact of the second. These effects included decreased SpO2 (overall Standard Mean Difference, SMD = 0.24, 95% CI = 0.38 to 0.11, p < 0.001) and minute ventilation (SMD = 0.72, 95% CI = 0.99 to 0.46, p < 0.001), simultaneous increased in blood-CO2 (SMD = +0.64, 95% CI = 0.310.96, p < 0.001), heart rate (N95: SMD = +0.22, 95% CI = 0.030.41, p = 0.02), systolic blood pressure (surgical: SMD = +0.21, 95% CI = 0.030.39, p = 0.02), skin temperature (overall SMD = +0.80 95% CI = 0.231.38, p = 0.006) and humidity (SMD +2.24, 95% CI = 1.323.17, p < 0.001). Effects on exertion (overall SMD = +0.9, surgical = +0.63, N95 = +1.19), discomfort (SMD = +1.16), dyspnoea (SMD = +1.46), heat (SMD = +0.70), and humidity (SMD = +0.9) were significant in n = 373 with a robust relationship to mask wearing (p < 0.006 to p < 0.001). Pooled symptom prevalence (n = 8,128) was significant for: headache (62%, p < 0.001), acne (38%, p < 0.001), skin irritation (36%, p < 0.001), dyspnoea (33%, p < 0.001), heat (26%, p < 0.001), itching (26%, p < 0.001), voice disorder (23%, p < 0.03), and dizziness (5%, p = 0.01).
Discussion: Masks interfered with O2-uptake and CO2-release and compromised respiratory compensation. Though evaluated wearing durations are shorter than daily/prolonged use, outcomes independently validate mask-induced exhaustion-syndrome (MIES) and down-stream physio-metabolic disfunctions. MIES can have long-term clinical consequences, especially for vulnerable groups. So far, several mask related symptoms may have been misinterpreted as long COVID-19 symptoms. In any case, the possible MIES contrasts with the WHO definition of health.
Conclusion: Face mask side-effects must be assessed (risk-benefit) against the available evidence of their effectiveness against viral transmissions. In the absence of strong empirical evidence of effectiveness, mask wearing should not be mandated let alone enforced by law.
This seems pretty intuitively obvious: wearing something in front of your nose and mouth all the time is probably going to block at least some of the virus from going in or out.
Intuitively obvious...and unscientific. Look at the slides presented by the industrial hygienist I linked to. Most of the virus is contained in aerosols which pass through the masks like a marble thrown at a building covered with scaffolding. And the aerosols are suspended and circulate in the air for hours. You do realize that surgical masks were never intended to stop the spread of airborne viruses, right?
Intuitively obvious...and unscientific. Look at the slides presented by the industrial hygienist I linked to. Most of the virus is contained in aerosols which pass through the masks like a marble thrown at a building covered with scaffolding. And the aerosols are suspended and circulate in the air for hours. You do realize that surgical masks were never intended to stop the spread of airborne viruses, right?
Ho-hum, just another day in the insane asylum...
Yeah, it was gain-of-function research funded by Fauci that caused millions of deaths
"But we also know this was not a natural disaster, this disaster was man made.
A list of genocides on Wikipedia shows that there have been no single human atrocities in the history of mankind that have come close to the deaths caused from the COVIDcrisis.
How do we "know this"? Because we have the receipts thanks to Judicial Watch, as well as the Congressional investigations - still ongoing.
This week, Judicial Watch received 552 pages from the U.S. Department of Health and Human Services (HHS). These documents include the initial grant application, biosketches, budgets and annual reports to the NIH from EcoHealth Alliance. They describe the specific aims of the project, which include creating mutant viruses SARS (and MERS viruses) "to better predict the capacity of our CoVs [coronaviruses] to infect people."
I spent the afternoon reading these documents and the 552 pages are a gold mine of information. But the specific aim 3 of the contract is particularly important. It reads in full:
Yeah, it was gain-of-function research funded by Fauci that caused millions of deaths
"But we also know this was not a natural disaster, this disaster was man made.
A list of genocides on Wikipedia shows that there have been no single human atrocities in the history of mankind that have come close to the deaths caused from the COVIDcrisis.
How do we "know this"? Because we have the receipts thanks to Judicial Watch, as well as the Congressional investigations - still ongoing.
This week, Judicial Watch received 552 pages from the U.S. Department of Health and Human Services (HHS). These documents include the initial grant application, biosketches, budgets and annual reports to the NIH from EcoHealth Alliance. They describe the specific aims of the project, which include creating mutant viruses SARS (and MERS viruses) "to better predict the capacity of our CoVs [coronaviruses] to infect people."
I spent the afternoon reading these documents and the 552 pages are a gold mine of information. But the specific aim 3 of the contract is particularly important. It reads in full:
Later, they write (page 195):Quote:
Specific Aim 3: Testing predictions of CoV inter-species transmission. We will test our models of host range (i.e. emergence potential) experimentally using reverse genetics, pseudovirus and receptor binding assays, and virus infection experiments in cell culture and humanized mice. With bat-CoVs that we've isolated or sequenced, and using live virus or pseudovirus infection in cells of different origin or expressing different receptor molecules, we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors. We will then use receptor-mutant pseudovirus binding assays, in vitro studies in bat, primate, human and other species' cell lines, and with humanized mice where particularly interesting viruses are identified phylogenetically, or isolated. These tests will provide public health-relevant data, and also iteratively improve our predictive model to better target bat species and CoVs during our field studies to obtain bat-CoV strains of the greatest interest for understanding the mechanisms of cross-species transmission.
It is important to understand that, although these quotes are technical and well beyond many to understand, the bottom line is that this project was and is gain of function research. In contrast to Dr. Fauci's sworn testimony to Congress."Quote:
we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors.
Might he face any consequences?
Zippergate said:
Ho-hum, just another day in the insane asylum...
Yeah, it was gain-of-function research funded by Fauci that caused millions of deaths
"But we also know this was not a natural disaster, this disaster was man made.
A list of genocides on Wikipedia shows that there have been no single human atrocities in the history of mankind that have come close to the deaths caused from the COVIDcrisis.
How do we "know this"? Because we have the receipts thanks to Judicial Watch, as well as the Congressional investigations - still ongoing.
This week, Judicial Watch received 552 pages from the U.S. Department of Health and Human Services (HHS). These documents include the initial grant application, biosketches, budgets and annual reports to the NIH from EcoHealth Alliance. They describe the specific aims of the project, which include creating mutant viruses SARS (and MERS viruses) "to better predict the capacity of our CoVs [coronaviruses] to infect people."
I spent the afternoon reading these documents and the 552 pages are a gold mine of information. But the specific aim 3 of the contract is particularly important. It reads in full:Later, they write (page 195):Quote:
Specific Aim 3: Testing predictions of CoV inter-species transmission. We will test our models of host range (i.e. emergence potential) experimentally using reverse genetics, pseudovirus and receptor binding assays, and virus infection experiments in cell culture and humanized mice. With bat-CoVs that we've isolated or sequenced, and using live virus or pseudovirus infection in cells of different origin or expressing different receptor molecules, we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors. We will then use receptor-mutant pseudovirus binding assays, in vitro studies in bat, primate, human and other species' cell lines, and with humanized mice where particularly interesting viruses are identified phylogenetically, or isolated. These tests will provide public health-relevant data, and also iteratively improve our predictive model to better target bat species and CoVs during our field studies to obtain bat-CoV strains of the greatest interest for understanding the mechanisms of cross-species transmission.It is important to understand that, although these quotes are technical and well beyond many to understand, the bottom line is that this project was and is gain of function research. In contrast to Dr. Fauci's sworn testimony to Congress."Quote:
we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors.
Judicial Watch has a long history of providing bogus one-sided information
fine, but these are FOIA'd documents and they don't have a history of faking FOIA's info.
They do have a history of selectively finding and releasing information. I'm just saying - I'm not an expert in this field and I'm not going to "do my own research". I'm going to listen to trusted sources and Judicial Watch is not that.MinotStateBeav said:
fine, but these are FOIA'd documents and they don't have a history of faking FOIA's info.
Zippergate said:
Ho-hum, just another day in the insane asylum...
Yeah, it was gain-of-function research funded by Fauci that caused millions of deaths
"But we also know this was not a natural disaster, this disaster was man made.
A list of genocides on Wikipedia shows that there have been no single human atrocities in the history of mankind that have come close to the deaths caused from the COVIDcrisis.
How do we "know this"? Because we have the receipts thanks to Judicial Watch, as well as the Congressional investigations - still ongoing.
This week, Judicial Watch received 552 pages from the U.S. Department of Health and Human Services (HHS). These documents include the initial grant application, biosketches, budgets and annual reports to the NIH from EcoHealth Alliance. They describe the specific aims of the project, which include creating mutant viruses SARS (and MERS viruses) "to better predict the capacity of our CoVs [coronaviruses] to infect people."
I spent the afternoon reading these documents and the 552 pages are a gold mine of information. But the specific aim 3 of the contract is particularly important. It reads in full:Later, they write (page 195):Quote:
Specific Aim 3: Testing predictions of CoV inter-species transmission. We will test our models of host range (i.e. emergence potential) experimentally using reverse genetics, pseudovirus and receptor binding assays, and virus infection experiments in cell culture and humanized mice. With bat-CoVs that we've isolated or sequenced, and using live virus or pseudovirus infection in cells of different origin or expressing different receptor molecules, we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors. We will then use receptor-mutant pseudovirus binding assays, in vitro studies in bat, primate, human and other species' cell lines, and with humanized mice where particularly interesting viruses are identified phylogenetically, or isolated. These tests will provide public health-relevant data, and also iteratively improve our predictive model to better target bat species and CoVs during our field studies to obtain bat-CoV strains of the greatest interest for understanding the mechanisms of cross-species transmission.It is important to understand that, although these quotes are technical and well beyond many to understand, the bottom line is that this project was and is gain of function research. In contrast to Dr. Fauci's sworn testimony to Congress."Quote:
we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors.
You pumped about the new coaching hires? It's finally got me hopeful for the first time in years for one of our major athletic programs. We can probably thrive in the small of the two major sports. Football will be tough.
My interest in Cal sports has declined dramatically in recent years. Decades of frustration and the dismal outlook have taken a toll, but the truth is I've become a huge fan of soccer thanks to my kids and now follow the European leagues pretty closely.
As for the new hires, I always had a great deal of respect for Madsen. Hopefully he can get things turned around. Cal should be able to compete a little in MBB, right? Hope springs eternal.
As for the new hires, I always had a great deal of respect for Madsen. Hopefully he can get things turned around. Cal should be able to compete a little in MBB, right? Hope springs eternal.
"You requested All reports submitted by EcoHealth Alliance to NIH or its sub-agencies related to
NIH Grant No. 1R01AI110964 titled "Understanding the Risk of Bat Coronavirus Emergence"
during the term of the grant. (Date Range for Record Search: From 04/01/2014 To 12/02/2021).
NIH searched their files and found 552 pages of responsive records."
Judicial watch released the entire file. 552 pages of records attached to a two-page cover letter.
They do have a history of selectively finding and releasing information. I'm just saying - I'm not an expert in this field and I'm not going to "do my own research". I'm going to listen to trusted sources and Judicial Watch is not that.
Not selective. I'm curious what you consider trusted sources and why you think Fauci did not perjure himself when he said he did not fund GOF research, a violation of federal law.
Who said I didn't think Fauci perjured himself?Zippergate said:
"You requested All reports submitted by EcoHealth Alliance to NIH or its sub-agencies related to
NIH Grant No. 1R01AI110964 titled "Understanding the Risk of Bat Coronavirus Emergence"
during the term of the grant. (Date Range for Record Search: From 04/01/2014 To 12/02/2021).
NIH searched their files and found 552 pages of responsive records."
Judicial watch released the entire file. 552 pages of records attached to a two-page cover letter.
They do have a history of selectively finding and releasing information. I'm just saying - I'm not an expert in this field and I'm not going to "do my own research". I'm going to listen to trusted sources and Judicial Watch is not that.
Not selective. I'm curious what you consider trusted sources and why you think Fauci did not perjure himself when he said he did not fund GOF research, a violation of federal law.
dajo9 said:Who said I didn't think Fauci perjured himself?Zippergate said:
"You requested All reports submitted by EcoHealth Alliance to NIH or its sub-agencies related to
NIH Grant No. 1R01AI110964 titled "Understanding the Risk of Bat Coronavirus Emergence"
during the term of the grant. (Date Range for Record Search: From 04/01/2014 To 12/02/2021).
NIH searched their files and found 552 pages of responsive records."
Judicial watch released the entire file. 552 pages of records attached to a two-page cover letter.
They do have a history of selectively finding and releasing information. I'm just saying - I'm not an expert in this field and I'm not going to "do my own research". I'm going to listen to trusted sources and Judicial Watch is not that.
Not selective. I'm curious what you consider trusted sources and why you think Fauci did not perjure himself when he said he did not fund GOF research, a violation of federal law.
Do you believe Fauci perjured himself because the NIH indeed funded Gain of Function research with Coronaviruses and Bats at the Wuhan Lab?
I don't know and I haven't expressed an opinion on it because I don't know. I haven't been following it all as many of you have. I jumped in here to point out that, for people like me, looking for information from trusted sources - Judicial Watch was not that.oski003 said:dajo9 said:Who said I didn't think Fauci perjured himself?Zippergate said:
"You requested All reports submitted by EcoHealth Alliance to NIH or its sub-agencies related to
NIH Grant No. 1R01AI110964 titled "Understanding the Risk of Bat Coronavirus Emergence"
during the term of the grant. (Date Range for Record Search: From 04/01/2014 To 12/02/2021).
NIH searched their files and found 552 pages of responsive records."
Judicial watch released the entire file. 552 pages of records attached to a two-page cover letter.
They do have a history of selectively finding and releasing information. I'm just saying - I'm not an expert in this field and I'm not going to "do my own research". I'm going to listen to trusted sources and Judicial Watch is not that.
Not selective. I'm curious what you consider trusted sources and why you think Fauci did not perjure himself when he said he did not fund GOF research, a violation of federal law.
Do you believe Fauci perjured himself because the NIH indeed funded Gain of Function research with Coronaviruses and Bats at the Wuhan Lab?
Why aren't their more interviews with U.S. citizens who were harmed by the COVID vaccines?
— KanekoaTheGreat (@KanekoaTheGreat) April 23, 2023
•65,253 Permanently Disabled
•26,823 Myocarditis
•15,647 Shingles
CDC VAERS reports are filed under penalty of perjury, and most are completed by medical professionals. pic.twitter.com/KxvJ4NeKfg
VAERS database shows 35,152 deaths from the Covid vaccine.
Complicit MSM, also young know-nothing journalists.
THREAD🚨 #SuddenlyCollapsed
— KanekoaTheGreat (@KanekoaTheGreat) January 13, 2023
Why are so many professional athletes and public figures collapsing live on television❓
•Damar Hamlin
•Sergio Aguero
•Jessica Robb
•Victor Lindelöf
•Heather McDonald
•Samuel Kalu
Here are 40+ sudden collapses since Jan. 2021: pic.twitter.com/a5zPaobB8a
The CEO of the OneAmerica insurance company publicly disclosed that during the 3rd and 4th quarters of 2021, death in people of working age (18-64) was 40% higher than it was before the pandemic.
Significantly, the majority of the deaths were not attributed to COVID.
From Feb. 2021 to Mar. 2022, millennials experienced the equivalent of a Vietnam war, with more than 60,000 excess deaths.
The majority of those deaths were not attributed to COVID.
Damar Hamlin collapsed after a brutal blow to the chest stopped his heart. If you're leading with that clear cut case that wasn't vaccine related (or at least had an EXTREMELY remote chance of being vaccine related), then it's hard to take the rest of your list and "facts" seriously.BearHunter said:THREAD🚨 #SuddenlyCollapsed
— KanekoaTheGreat (@KanekoaTheGreat) January 13, 2023
Why are so many professional athletes and public figures collapsing live on television❓
•Damar Hamlin
•Sergio Aguero
•Jessica Robb
•Victor Lindelöf
•Heather McDonald
•Samuel Kalu
Here are 40+ sudden collapses since Jan. 2021: pic.twitter.com/a5zPaobB8a
The CEO of the OneAmerica insurance company publicly disclosed that during the 3rd and 4th quarters of 2021, death in people of working age (18-64) was 40% higher than it was before the pandemic.
Significantly, the majority of the deaths were not attributed to COVID.
From Feb. 2021 to Mar. 2022, millennials experienced the equivalent of a Vietnam war, with more than 60,000 excess deaths.
The majority of those deaths were not attributed to COVID.
By the way, I hear Hamlin has not only recovered, he's been cleared to play football again.
Featured Stories
See All
Bear Insider Cal Weekly Grab Bag – August 7, 2026
by Scott Butler
Cal Football Media Day Roundup
by Jim McGill
Bears Kick Off Fall Camp at Memorial
by Jim McGill
Media Day: Lupoi on New Role, Recruiting, Season Expectations
by Ian Firstenberg