Unit2Sucks said:
Cal88 said:
Unit2Sucks said:
Cal88 said:
smh said:
front page of sunday's nytimes top to bottom / left to right (continued on page 12) is given to the dead.
Quote:
Departments across The Times have been robustly covering the coronavirus pandemic for months. But Ms. Landon and her colleagues realized that "both among ourselves and perhaps in the general reading public, there's a little bit of a fatigue with the data."
"We knew we were approaching this milestone," she added. "We knew that there should be some way to try to reckon with that number."
Putting 100,000 dots or stick figures on a page "doesn't really tell you very much about who these people were, the lives that they lived, what it means for us as a country," Ms. Landon said. So, she came up with the idea of compiling obituaries and death notices of Covid-19 victims from newspapers large and small across the country, and culling vivid passages from them.
Alain Delaqurire, a researcher, combed through various sources online for obituaries and death notices with Covid-19 written as the cause of death. He compiled a list of nearly a thousand names from hundreds of newspapers. A team of editors from across the newsroom, in addition to three graduate student journalists, read them and gleaned phrases that depicted the uniqueness of each life lost:
"Alan Lund, 81, Washington, conductor with 'the most amazing ear' "
"Theresa Elloie, 63, New Orleans, renowned for her business making detailed pins and corsages "
"Florencio Almazo Morn, 65, New York City, one-man army "
"Coby Adolph, 44, Chicago, entrepreneur and adventurer "

Last winter, 80,000 Americans died from the flu, and the NYT barely noticed.
CDC: 80,000 people died of flu last winter in U.S.
I guess that reporting that the death toll from flu viruses this year is 25%-35% above last year's doesn't make as dramatic a headline.
That wasn't this year. This year the estimates are 24-62k. I'm not sure how relevant it is to refer to the flu - we do have a flu vaccine that people can take which helps reduce mortality annually, so it's not like we ignore the seasonal flu either.
We have good flu years and bad flu years. That is neither here nor there when discussing a novel virus like COVID.
Why the misinformation?
Look at what you posted 2 months ago about COVID and please let us know why you are singing a completely different tune now.
The 80,000 US deaths from the flu was from the 2017-18 season, OK, not the 2018-19. This doesn't change my main point about the covid-19 mortality looking more like a very bad flu season, around 50% worse than the flu season from 2 years ago, rather than the kind of extraordinary pandemic most observers feared it was two months ago.
So we now know that the C19 fatality rate is far lower than previously estimated. Initially the WHO has put that figure at up to 3.4%, while the recent CDC estimates have been revised downwards closer to the seasonal flu envelope
The picture we had 3 months ago, shown below, which I was the first to post on this board, turned out to be way too alarmist:

This is the data released by the CDC two months later in May back when the death toll was 74,000:
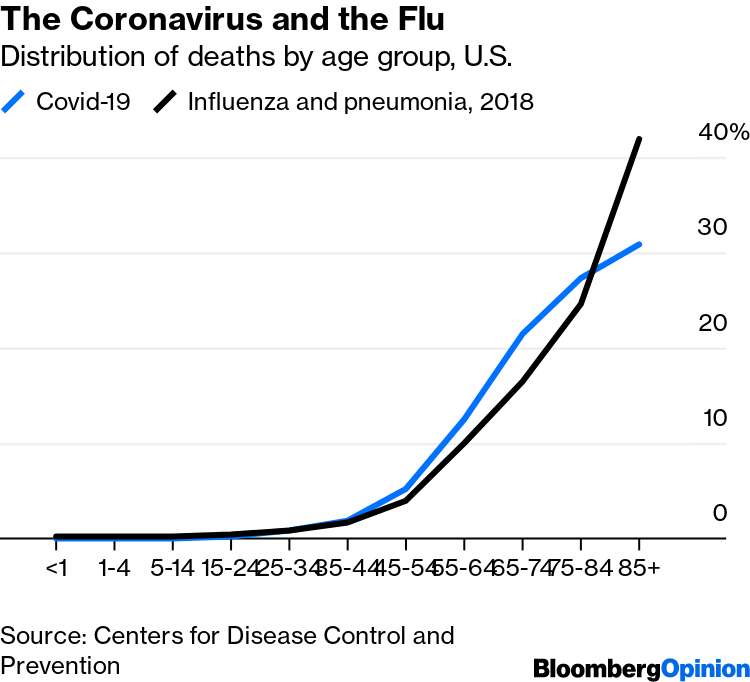
We're headed to a total in the 130k-140k range, so the blue curve above will shift up, but it will still be of the same order of magnitude, about twice as bad as a recent bad flu season, of the order of the 1957 Asian Flu and the 1986 Hong Kong Flu, both of which ha a death toll in the low 100,000s. We are nowhere near the Spanish Flu as some alarmist modelers like Imperial College's Ferguson have predicted.
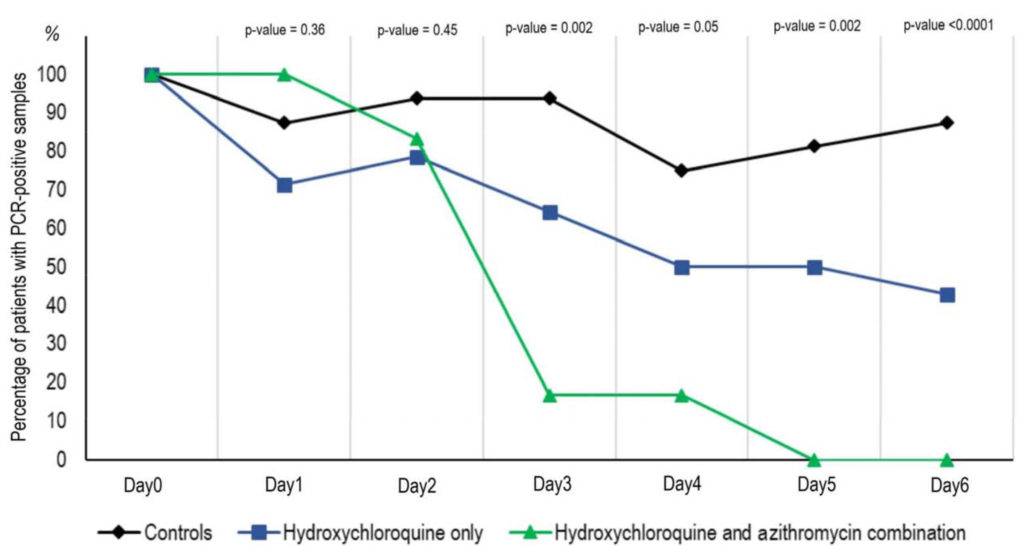
Furthermore,we now also have treatments like the HCQ/Azythromycin/zinc regimen, which gas proven to be highly effective in reducing the viral loads and death rates if applied under the right protocol in the early to middle stages of the disease (as opposed to the later stage, where the virus is no longer the main pathology agent).
This is the treatment that is being used successfully in dozens of countries around the world, including India, Israel, Russia,Turkey and over a dozen African countries, all of which have had great success using HCQ with the protocol fine-tuned by Dr Didier Raoult in his Marseille hospital. The recent Lancet study that claimed HCQ was ineffective has now been thoroughly discredited.
Thanks for answering and acknowledging that you said this year's flu but actually referred to 2 seasons ago. This year's flu killed between 1/4 and 1/2 as many as COVID already has. And the deaths are incremental - it's not like we get to choose between one or the other. I do wonder whether SIP helped reduce normal flu deaths by limiting spread. I suspect we will find out.
Few other thoughts in response.
First - the second chart doesn't speak to magnitude. It's speaks to relative death mix. COVID could kill 2 million and the chart wouldn't move. So it may be interesting but it's not particularly relevant when discussing magnitude of mortality of flu or COVID.
Second - you said your prior data was alarmist without acknowledging that SIP and social distancing are largely the reason we don't have far more dead. It's like saying we don't need seatbelts because people aren't dying from flying through windshields any more. It's not a coincidence. I suspect given the increase in new cases and hospitalizations we are seeing, combined with the relaxing of social distancing efforts, we aren't going to see mortality get close to zero for quite some time and that 140k will just be a waypoint in our battle. Would be surprised if we end up with fewer than 200k dead before year end and 250k by March 2021 (fully year into the pandemic). That would put COVID as a top 5 killer in the US over that 12 month period. Some of those people would have died anyway but it will be a major cause of excess deaths as well.
Third - you are just picking and choosing on HCQ like many others. I don't believe you ever responded to my critique of the Marseilles HCQ results that you crow about but it's quite apparent that they were misleading. Now you are basically saying HCQ is helpful for people who will probably do fine no matter what. It's not an apples to apples comparison. The vast majority of people in the early stages of the disease will do just fine. Many who won't are ineligible for HCQ due to the risks of side effects and those are the people most at risk. In Merseille they had to cut out more than 1/4 patients from the trials because of these risks and those at risk patients are the ones who most would benefit from a therapy. HCQ is unlikely to be the reason mortality has been reduced anywhere. I think others have posted on the Lancet study, but to be clear it hasn't been rebuked. It was withdrawn because they didn't have permission to allow the data to be reviewed. It should have been withdrawn but that doesn't mean that it was invalid rather that it just couldn't be peer reviewed.
I would love more than anything for HCQ to be a silver bullet here but that is just hard to justify right now given how many studies have shown otherwise.
Perhaps one takeaway from what you now acknowledge was an incorrect and alarmist view in February is that you shouldn't be so confident in your predictions.
We know a lot more about the disease now than we did back in February. I was correct in predicting the pandemic's arrival in the US all the way back in February, and the disruption it would cause, and was widely mocked for that and dismissed as some king of prepper. If you have the same mindset today that you did in March, it indicates you haven't incorporated many basic facts about the disease that we've learned along the way.
There are too many points to refute here and not that much time, I will just stick with a couple of very glaring points that show that you have a completely false understanding of what HCQ is about.
Quote:
Many who won't are ineligible for HCQ due to the risks of side effects and those are the people most at risk. In Merseille they had to cut out more than 1/4 patients from the trials because of these risks and those at risk patients are the ones who most would benefit from a therapy.
The side effects from HCQ over the short term in the right dosage (1) are very well known and documented, as the drug has been prescribed/used
over a billion times across the world and (2) are very benign over the short term. HCQ has been an OTC drug for decades.
Any pharmacist or physician from countries where this drug is commonly administered would laugh at the notion that this drug is dangerous. The fact that this notion is so widely spread in American circles indicates that the general public here is grossly misinformed, which is perhaps a symptom of the very polarized political environment we live in. If you can't get this fact straight about HCQ side effects, we're just not going to go very far in this discussion.
Quote:
I think others have posted on the Lancet study, but to be clear it hasn't been rebuked. It was withdrawn because they didn't have permission to allow the data to be reviewed.
That's a gross mischaracterization, the three authors of this study retracted their names from the study because they could not vouch for the authenticily of the data used. The data provided by Surgisphere, the fly by night company that was supposed to gather the data, is outright fraudulent, for example it showed more deaths in Australia from HCQ treatments than the actual total number of covid deaths in that continent, and abnormalities like little variations across continents in the profile of the data.
Fact checkers from reputable media sources contacted over 100 hospitals that were supposed to have provided their data to the study, none of their officials even knew of Surgisphere. It's not that they had confidentiality clauses with Surgisphere, it's that they have unequivocally stated that they've never even heard of them.
Another negative study on side effects of HCQ recently published by the N England Journal of Medecine from the same team with Mehta, using Surgisphere data, was also rebuked by the magazine, who issued an
"expression of concern" about the study and the data used.
Quote:
the second chart doesn't speak to magnitude. It's speaks to relative death mix. COVID could kill 2 million and the chart wouldn't move.
We're well past the peak in the US in covid deaths. The notion that it could still kill a million or two here is ridiculous, the total will be in the low to mid 100k range.
We know this because this is what happened in other countries with similar death rates, it's the basic behavior of all viral respiratory epidemics, the national aggregates of new deaths are bell curves with wider tapering, that's true in every country, and it will be true in the US.